Beyond Butt Wink: Hip Shape, Injuries, and Individual Ability Part 1
A few months ago I wrote an article on how Butt Wink, that fun little tuck under at the bottom of some peoples squats, had next to nothing to do with the hamstrings, and it was very well received. For those who don’t want to check out the article, I’ll tl:dr that sucker:
Your hip shape says more about your butt wink than your hamstring tension.

A lot has been made about how bone shape means you have to squat differently. This article on the PTDC did a great job at inferring from the anatomical differences that squat stances and depths should be different, but aside from basic inference, there’s not a lot that’s been written about the actual research into the topic. I wanted to change that. This series is going to look at the essential research that’s look into joint type, alignment, and wear patterns, as well as ranges of motion affected from the different alignments, plus show how to assess and determine what training directions you should take for your specific anatomy.
Anatomical Differences
Many training programs assume hip structure and geometry are constants, meaning everyone has the same bone and joint angles and positions. We know by looking at two different people, maybe a female gymnast and a male football center, that their specific anatomy is bound to be different. Likewise, the football center may never be able to move like the gymnast, not through any fault of their own but simply because they are built differently.
Zalawadia et al (2010) showed there’s a big variance in the femoral anteversion angle (whether the head of the femur pointed more forward or possibly backward) as the femoral neck attaches to the acetabulum, with the majority being between 10-20 degrees.
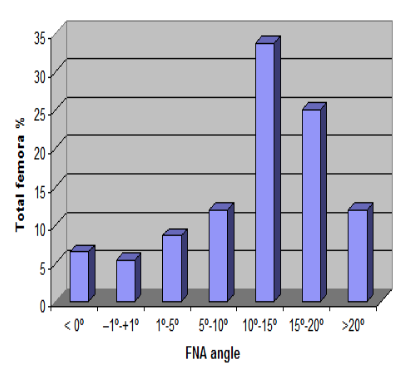
This range accounted for about 55% of people tested, but that means there’s still 45% of people not within that range.
Higgins et al (2014) even showed there was a large difference in anteversion angles bilaterally in the same individual, potentially lending some validity to PRI concepts of inherent asymmetry.
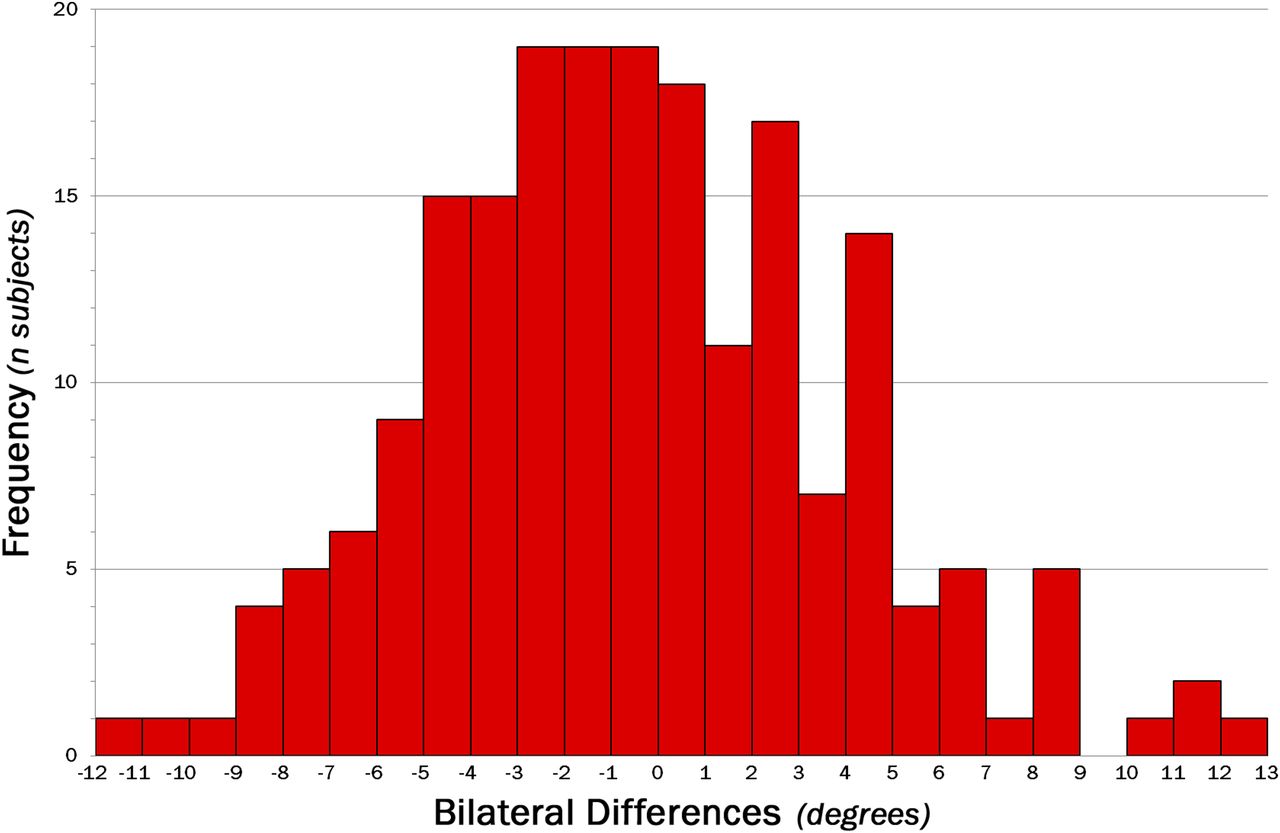
Frequency and magnitude of intrapatient bilateral differences for anatomic anteversion (left side minus right), showing relative symmetry.
In terms of the acetabular angle, D’Lima et al (2011) found in a computerized prediction model for prosthesis implantation that those with more acetabular anteversion (forward placement on the pelvis) had greater flexion range of motion and less extension, lateral placement of 45-55 degrees gave the best overall mobility, but a lateral angle of less than 45 degrees gave more flexion range of motion and more than 45 degrees gave less rotation capability. He even showed that if the femoral neck was thicken by 2 mm in diameter it significantly reduced the range of motion in all directions, irrespective of placement.
So we know there’s a broad difference in hip structures and how they can potentially move. One of the common concepts of trying to create movement beyond the structural ability is the butt wink, which would predispose the low back to moving more than necessary during a deep hip flexion movement, but another is femoral acetabular impingement, or FAI. This is where the bony ridge of the acetabulum presses into the femoral neck and creates irritation that eventually leads to bone growth and pain when the bones are further compressed into each other. I’d even wager to say that FAI was present in cases of butt wink during deep squats too.
Frank et al (2015 epub ahead of print) showed a good-sized percentage of the population had asymptomatic FAI present on radiographs. 37% of subjects scanned had cam deformities (where the femoral neck gets thickening from compression), and that sub-group went up to 54.8% in athletic individuals, and a whopping 67% of subjects had a pincher deformity (where the acetabular ridge develops a bony callous), again higher in athletes with 71% of the sub-group.
Now if acetabular anteversion (more forward placement of the cup) showed increased flexion range of motion, a retroversion position would decrease that flexion and likely increase the risk of compression injuries that would result in FAI. Fabricant et al (2015) showed exactly that when he connected retroverted acetabulums with decreased clinical outcomes in FAI patients.
Hip angles don’t just affect the range of motion at the hip. Major joints usually have a direct impact on joints next to them, and the SI joint is the closest to the hip. Morgan et al (2013) showed that symptomatic SI joint patients had some similarities in their radiographs. 33% had cam deformities, 47% had either deep hip sockets or medial protrusions into the pelvis.

For cases of FAI, it could be said that the causative factor was pushing the joints into a range of motion outside of their own structural abilities. For the SI joint issues, a contributing factor could be similar, although not the sole cause of the dysfunction. Therefore it could be said that in some people, training in a theoretical “full” range of motion could be the worst thing they could do for joint health. In many cases, these ranges of motion will be further limited with age as joint degeneration and spacing is further reduced. Trying to force a range of motion that will not happen willingly is a recipe for disaster.

Having the goal of showcasing a bullet-proof squat is admirable, but in many cases will require you to pick your parents appropriately before beginning the workout program. The good thing is that a negative in one light is a positive in another. If someone doesn’t have the hip structure to allow deep hip flexion, they often may have great hip extension. If they have deep sockets, their chances of developing stabilization overuse injuries through the hips are minimal, which means weight bearing activities and impact drills (as well as running) would be very well tolerated. One term I heard a long time ago from a workshop attendee was “You’re either squatting or storming” referencing the ability of military personnel to march long distances with full packs and weaponry and storm a castle. It was brilliantly simple.

The recipe for deep squatting seems to be slight femoral anteversion combined with acetabular anteversion, lateral placement of less than 45 degrees, and a thin femoral neck. People with this configuration have the ability to drop into a deep squat without any real issues, irrespective of muscle force, tension or capsular restrictions. Those still have contributions, but looking purely at structure, this seems to be the best scenario.
So the obvious question would be how do you determine your own hip structure and what would be your ideal range of motion for different activities like flexion or extension? We’ll cover that in part 2 next day.
3 Responses to Beyond Butt Wink: Hip Shape, Injuries, and Individual Ability Part 1