Stretching Isn’t Bullshit
Todays post comes from Jasper De Coninck, a Belgian physio who also has experience with strength training. Enjoy.
*****
[Disclaimer: For the laymen, who are just interested in the essence of the article and whether to stretch or not to stretch, short summaries are in the underlined centered sentences.]
Stretching is quite the controversial term in the fitness community. In one corner, you have the functional crowd putting stretching on a pedestal and spending an hour a day stretching away in sizzling positions. In the other corner, you have team barbell advocating strength training with full range of motion: “that’s all that’s needed”. It’s time to get some ropes out, draw a line in the sand and settle this tug of war.
A little intro…
In the literature, there are several terms coined to get a grasp of what mobility entails. In his book “Movement” (7), Gray Cook uses the pyramid of movement patterns upon stability upon mobility. To completely own a movement pattern, you need the necessary stability over a certain range of motion. If you’re able to display this active range of motion in other patterns, only learning the movement itself remains. This pure simplicity is both its strength and downfall at the same time. Other systems make it more complicated by drifting further away from an ordinal view. They see mobility more on a continuum.
“Stability is control of a joint system in the presence of change” – Charlie Weingroff
Stability is preventing a fixed point from moving by producing the strength to counteract movement over a certain range of motion. This makes it a certain type of strength. Active mobility, as in displaying change under presence of stability, is strength in a specific mobility. This makes it, again, a form of strength. The range you can’t control is termed passive range of motion. Active mobility should be the end goal of all stretching routines. Increasing passive range of motion, without being able to demonstrate you have strength through this range, will only increase the odds of getting injured in that range.
Your mobility can be limited by several possible culprits. All these possible factors can be put in one of 2 buckets: a structural or a functional bucket. A structural limitation is an actual limitation of the tissue. A functional limitation is the nervous system (NS) not granting mobility through a full range of motion.
A non-exhaustive list:
| Structural | Functional |
| Articular capsule | Threat |
| Muscle length | Perception |
| Skin | ANS response |
| Nerves | Readiness |
| Connective tissue | Alignment |
| … | … |
It is paramount to make a clear distinction between the two. Bringing change to the functional bucket will be rapid and look like magic. Messing with the structural bucket… not so much. The McKenzie system divides impairments and disorders into fast or slow responding for a reason. This rehab system is based upon repeating specific motions.
In a nutshell, you can reacquire your structural mobility from your functional mobility quite rapidly by giving the right input. Once it’s there, to get any additional range, you need to alter the tissue which is limiting the mobility. That takes force over time.

Structural mobility
Whether stretching can be used to alter the tissue structurally is still a bit up to debate. A study by Antonio & Gonyea et al showed that prolonged weighted stretching in birds has the potential to actually alter the muscle length of the tissue. In the past, prominent authors such as Shirley Sahrmann have written about alterations in muscle length by protocols lasting more than 30 minutes in symptomatic individuals. The idea is based upon a review in which the authors concluded: “though this current information is from animal studies, clinical observations and preliminary investigations suggest its applicability to humans”. Putting stretch on a muscle for a weally, weally long time thus alters the muscle length in animals.
The amount of force that’s needed to structurally stretch out surrounding tissue is absurd. Take fascia as an example. It is too stiff to alter its length without using considerable force. By considerable, think about chaining it up to a 4×4 and putting the jeep in S-mode. A recent review by Weppler et al studied the length/tension relationship of the muscles, before and after stretching in humans. If the length of a muscle changes after a thorough stretching protocol, tension would have to change accordingly. The review found this was simply not the case. For most muscles, it’s even biomechanically impossible to stretch to their full biomechanical length, with biarticular muscles like the hamstrings or the gastroc being the exception.
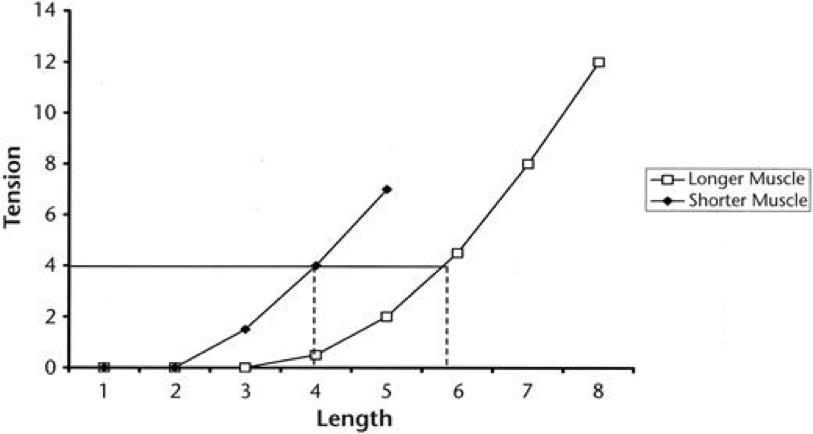
Figure from Weppler et al: The length-tension relationship changes when a muscle structurally lengthens.
Other modalities have shown to be able to alter this length-tension relationship. Brughelli et al reported several studies which showed a shift in optimum length after eccentric exercise. The authors note this could be indicative of an increase in the number of sarcomeres in series, i.e. actually lengthening the muscle. This would alter the length-tension relationship of the muscle as a whole. Since the eccentric is just an inherent part of dynamic resistance training, team barbell does have its first strike.
In conclusion, putting the tissue under load, with an enormous volume, gives a stimulus big enough for muscle length to alter in animals or in vitro. It doesn’t seem possible in humans though, by just stretching. Perhaps, the dose-response to structurally alter muscle length is not being replicated in the studies or is just beyond what is feasible to sustain by any human being. It definitely would be extremely time-intensive and not really practical. Additionally, muscle length doesn’t seem to be the limiting factor in asymptomatic individuals. Maybe static stretching is only applicable to impairments or disorders where muscle length is actually altered, which seems to relate to the paramedical observations in the literature. In any case, the cost-benefit analysis for stretching to structurally alter tissue length is just not overly convincing to say the least.
Now, this doesn’t mean there isn’t any benefit to increasing the neural stretch tolerance. Increasing visco-elasticity and lowering the stretch reflex without gaining strength over the range of motion would make stretching a bit of active recovery. Because you’re not really changing anything, perhaps this time is better spend doing actual dynamic movements or training. This would mean you spend more time in the eccentric part. The real key is to learn how to display strength at an increased range of motion. Ranges where you can display strength are functional, which brings us to the next bucket.
Functional mobility
We already established that stretching is not your end all and be all to change tissue length. What about changing functional mobility? A lot of different modalities can be used to alter your functional mobility. Stretching is also one of them. The trick is to convince your nervous system to release fascial and muscular tone by lowering the perception of pain, increasing the neural stretch tolerance and lowering the visco-elasticity. If your structural mobility is at par, simply regaining full functional mobility can give you the prerequisites to perform a certain movement without compensation or to lower the perceived threat and become pain-free.
Actually, stretching is more closely related to strength training than you would imagine. Warm-up sets or going through the motions of a hard resistance training set can convince the nervous system to grant additional mobility. This is fundamentally not very different from stretching. Stretching is also an eccentric to get in the position with a prolonged kind of isometric and a concentric to get out of it. Rapid alterations in intra-muscular or intermuscular recruitment can change mobility. Altering rate of firing by irradiation can grant mobility in an otherwise passive range. Altering the function of proprioceptors can grant additional mobility (e.g. the gogli tendon organs becoming less sensitive after subsequent contractions or stretch). These are the same factors that bring about gains in strength in the short run. Movement stays movement. Mobility is more closely related to strength training than you would think.
Stretching really shines when we need to alter functional mobility to get out of a dysfunctional pattern. That is how you can regain your physiological structural mobility rapidly.
A textbook example is a difference in straight leg raise left to right with an anteversion of the ilium on one side. In this case it could be a fibrotic adhesion within an anterior structure which is actually anteverting the ilium and inducing the difference in function. When stretching the posterior “tissue stuff” to become symmetrical, problems will only get worse because you’re feeding the dysfunction. When stretching out of the dysfunction, often mobility is gained in a multitude of directions. On top of that, another underlying structural mobility for which the body was compensating can surface. If we were to look at it from Cook’s model, most of the time stability is already there, underlying a non-painful mobility dysfunction.

Figure: Anteversion of the left ilium due to an anterior restriction. As a consequence, left straight leg raise will be limited.
We normally expect these rapid changes to be a transient improvement, which we have to load or reinforce, to engrain permanently. This isn’t always necessary. A recent paper by Pietrzak et al confirms the above paragraph by bringing the modified long slump sit (MLSS) back to live. In the past, the MLSS was introduced by Nev Austin, but nobody picked it up. In the study, the subjects did the neurodynamic stretch for only 1 session with 3 sets of 5 repetitions of 5 second holds. They all had a passive straight leg raise below 75-80° and were allocated to either stretching the dominant leg or the non-dominant leg. They refrained from any stretching until the follow-up. After 3 weeks, the authors concluded: “unilateral MLSS application significantly improved bilateral segmental (hamstrings; ipsilateral > contralateral) and extra-segmental (rectus femoris; ipsilateral = contralateral) muscle extensibility and stretch tolerance, which was retained 3 weeks post-intervention.” In english: “Subjects retained their increased leg raise after 3 weeks with just one stretch session. Even better, mobility was gained in other directions as well, on both sides.” This means the mobility improvement wasn’t limited to the stretched tissue. Rec fem muscle extensibility increased without stretching the muscle. The added neurodynamic component did seem to alter the perception of stretch effectively, which is perhaps why the subjects could retain the gained mobility long term.
There can also be quite some overlap between structure and function. Imagine a patient with neurogenic tightness in his piriformis due to a disc herniation. His piriformis will be functionally limiting complete mobility of the hip. By treating the structure, the intervertebral disc in this case, you will be able to increase the stretch tolerance of the piriformis and thus increase functional mobility. Another example is the one with the anteverted ilium we encountered earlier (sounds like a Friends episode). Getting the pelvis back to neutral alters its alignment and consequently influences the rotation of the spine. This could solve closing angle pain of the lumbar facet joints with rotation or extension. This also implies you can bring about structural mobility issues when stretching into dysfunction. Feeding the dysfunction by increasing the faulty pelvic alignment can increase the lumbar impingement. A functional mobility problem of the anterior tissue of the hip gives a structural mobility issue in the lower back.
The verdict on stretching?
The answer, as usual, is… it depends. How about that for a non-sexy answer? Stretching is a great tool in your toolbox to use on the right occasions. Stretching just to stretch is nonsense and time better spent on active recovery via other modalities. Whether somebody is drawn to or repulsed by stretching is usually a reflection from their past success and failure with the modality.
Most of the time, it depends on the actual underlying cause of their mobility restriction. Stretching can be very useful to fix a dysfunctional mobility problem. Just be sure you don’t stretch into dysfunction and you alter alignment for the better. It won’t have the same lasting effects when passively stretching to alter tissue with the goal to increase structural mobility.
Increasing mobility by changing the tissue = no-no
Regaining structural mobility by changing nervous system function = yes-yes
If you think about it, it seems both the functional and the strength crowd are right in this case. They are just talking about a different beast. If we view it from the right perspective, we are all tugging on the same side of the rope, without even knowing it.
ABOUT THE AUTHOR

Jasper De Coninck is a Belgian physio and strength coach with a main focus on the athletic population. He has a MS in sports and rehab and prides himself in constant education. His main specialties are mobility, movement based therapy, structural balance and weakness correction.
Website: www.rehabrevolution.org (under construction)
2 Responses to Stretching Isn’t Bullshit