Foam Rolling Isn’t Stretching, But It’s Still Important
A lot of controversy has developed as to what exactly is happening when you use a foam roller in terms of what is actually happening at the near cellular level to allow for new range of motion, and whether rolling itself is even necessary or potentially harmful. Personally and anecdotally, I roll and get my clients to roll because it works. You can see rather immediate increases in range of motion, better joint control for things like reduced valgus collapse in squats and less anterior weight shift following rolling of the IT band region, and improved shoulder mechanics for overhead movements with targeted work to the serratus region, and the only side effects seem to be immediate emotional trauma.
The biggest problem seems to be with understanding how range of motion could increase without taking a joint or joints through a larger excursion. Most flexibility programs involve hanging out at the end range of motion for various lengths of time, and while I’ve already shown this isn’t all that effective compared to other methods, it’s still a prevailing thought process.

Doing this won’t kill you, but it also won’t get your hammies longer either
For a muscle to become more flexible, one of two things (and ideally both) have to happen. First, you have to add more sarcomeres, the basic unit of a muscle, in series. This is like the old Barrel of Monkeys toy we all had as kids, where we would shake the small barrel with plastic monkeys and see how long of a train of monkeys we could pull out of the barrel at once without breaking. My personal record was 12. 
More sarcomeres in series = longer muscles. Another method is to involve using more range of contraction through each individual sarcomere. Considering the sliding filament theory, a muscle in a state where more fibers are bound and in a shortened position will cause the entire sarcomere to hold a shorter length, which means a tighter muscle. Stretching a muscle to a lengthened sarcomeric position involves having fewer interconnections within the microfilaments, which means a weaker muscle, but also the potential for either injury or instability. Chronically “tight” people are usually folks who have their muscles in a shortened position and an always “on” drive from the nervous system holding it there. Stretching will never overcome this nervous system drive to have a shortened muscle as there isn’t enough stimulus to override it.
[embedplusvideo height=”367″ width=”600″ editlink=”http://bit.ly/1ydb24z” standard=”http://www.youtube.com/v/0kFmbrRJq4w?fs=1″ vars=”ytid=0kFmbrRJq4w&width=600&height=367&start=&stop=&rs=w&hd=0&autoplay=0&react=1&chapters=¬es=” id=”ep3160″ /]
When the nervous system is not reducing the neural drive to cause the muscle to contract, the sodium and calcium gates get locked in the “on” position, one reason why rigor mortis causes the muscles to become rigid following death, but eventually become slack again after a few hours once the calcium and sodium channels have depleted.
The nervous system is one of the biggest guardians of the musculoskeletal system due to it’s desire to prevent you from demolishing yourself with contractile and guarded tension. You could easily over stretch and rip a muscle apart if left to your own devices, which is why the nervous system tends to over react and err on the side of caution.
So how does this have any impact on stretching and increasing range of motion, especially through foam rolling? Well, foam rolling doesn’t move the muscle through a larger excursion, which means you’re not stretching the sarcomere to a new position where it has to still allow some connections without ripping, and also doesn’t produce new sarcomeres in length, especially after 20 seconds of foam rolling. The process takes a lot longer to occur, like minutes or so, but who has time for that? (sarcasm, yo).
Now about what foam rolling is not.
A lot of people talk about fascia, myself included, which is an incredibly important tissue to understand and see how it works and moves. Rolling does a great job at compressing and stimulating the neuroreceptors of the fascia, but it doesn’t stretch it since the tissue isn’t moving in a proximal/distal manner to produce length changes. The compression causes a very minor length change under the weight of the body on the roller, but it’s incredibly minimal.
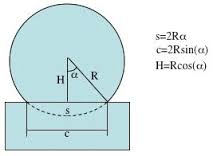
In this example, the difference in length between C (uncompressed distance) and s (compressed distance) is pretty minimal, and the only actual length change occurring in the roll. It’s akin to walking a distance on flat versus walking the same horizontal distance with a 1% incline and saying you walked further. Over the span of 5km, you probably added another 50 meters, which takes olympic sprinters about 5 seconds to cover. Not too sufficient.
If we were to take a different angle and technique on the manipulation of fascia, as is used in something like massage, ART, tool assisted therapies, you could see some noticeable change in length, but the majority of the effect on fascia and muscle is minimal sine much of this force application is lost through the superficial layers not transmitting that force to the end tissues and creates more shear force between the layers. When you see someone leave an aggressive session of soft tissue work with immediate bruising, the obvious impact was more to ripping the blood vessels apart and irritating the hell out of the skin.
 Odds are that tissue damage to this extent will cause some reciprocal guarding, and actually reduce the range of motion through the tissue more than increasing it, at least until the tissue irritation has healed up a little.
Odds are that tissue damage to this extent will cause some reciprocal guarding, and actually reduce the range of motion through the tissue more than increasing it, at least until the tissue irritation has healed up a little.
To get any force to the muscles and myofascia, you have to press pretty deep and hard in some stretched out positions to make sure you have enough grip on the area to cause some change. The superficial layers are pretty aqueous and squishy, and if you have someone who has some considerable adipose tissue it’s going to be tough to get deep enough to cause some damage. On top of that some of the compression will stimulate pain reception before the muscle or deep fascia is even touched, so the force application will be limited there.
 Foam rolling applies compressive force, not shear force (unless you get a little Tantric with the roller), and as a result it won’t be able to create the separation between layers, which is necessary to “break up” tissue adhesions or create a stimulus to reduce scar tissue. Now scar tissue is NOT something that smacks up on the IT band after you run a 5km run for the first time in 6 years, unless you had surgery or developed some nasty road rash after slipping on the ice. You developed DOMS, and probably some overactive neuroreceptors that have caused you to hate life.
Foam rolling applies compressive force, not shear force (unless you get a little Tantric with the roller), and as a result it won’t be able to create the separation between layers, which is necessary to “break up” tissue adhesions or create a stimulus to reduce scar tissue. Now scar tissue is NOT something that smacks up on the IT band after you run a 5km run for the first time in 6 years, unless you had surgery or developed some nasty road rash after slipping on the ice. You developed DOMS, and probably some overactive neuroreceptors that have caused you to hate life.
I’ll just put the soap box away now. Thanks for listening.
So let’s discuss what foam rolling MAY actually do. Please keep in mind that these are just my opinions of what happens and have some scientific backing, but they have not yet been proven.
Within the muscle there are neuroreceptors that sense length changes and positional velocities. The big guys are the golgi tendon organs and muscle spindles. They sense whether a muscle is stretching rapidly and cause some reflexive contraction and also whether force production in the muscle is too much and may cause some internal injuries. You see these stimulated when the doctor whacks your knee to test your reflexes.
Additional to these are some of the fascial receptors, which respond in a similar way but in a much slower manner. There’s actually 17 different types of fascial receptors which sense everything from temperature to joint angle, even down to what the concentration of oxygen in the blood is as it enters the tissues. The big length tension ones we can talk about here are the ruffini fibers and the pacini fibers. These work in a similar way as the golgi tendon and muscle spindle, but over a much longer and slower timeline.
When you use a foam roller and hit an area where these receptors are hyper sensitive, you’ll feel a ball of muscle contraction in a very small space. These hyperactive sarcomeres are working overtime because they’re essentially locked in the “on” position.

When you compress these hyperactive segments, it creates an overload on the receptor as the nervous system slams the neuromuscular connection with more stimulus to try to shake off the compressive element and avoid the pain and trauma. If there’s too much compression it can cause the muscle to contract harder, but enough compression to cause some overload can help stimulate and then fatigue the receptor, which helps to “release” the muscle or sarcomeres affected so there’s less tension. From the sliding filament theory, this helps to expand the length of the sarcomere, allowing more range of motion to occur.
This is a similar mechanism to PNF style stretching, where a muscle is stretched into a near end range position, then contracted in a held position for a time (usually 10-20 seconds), and then tension is reduced which then produces new range of motion.
[embedplusvideo height=”367″ width=”600″ editlink=”http://bit.ly/1ydSCAH” standard=”http://www.youtube.com/v/BJl5uPhWM6U?fs=1″ vars=”ytid=BJl5uPhWM6U&width=600&height=367&start=&stop=&rs=w&hd=0&autoplay=0&react=1&chapters=¬es=” id=”ep1954″ /]
This excitation-fatigue response is a common one when involving the nervous system and it’s effects on tension. In one instance, I had a client who during an initial assessment had a grand maul seizure, which was freaky enough on its’ own. However following the seizure, this client said she felt looser and proceeded to put both of her hands on the ground whereas before she could only get to her mid shins. We didn’t continue with the assessment as this warranted some medical attention.
**PLEASE NOTE** Before anyone goes on to the interwebz and says “OMG Dean recommends seizures for increasing range of motion,” I don’t. This was a one time incident that I mention to illustrate the possibility of neural tension development causing muscular inflexibility. If you have seizures, get that checked out and don’t consider this a viable way of getting your mobilities on, mkay??
When working on self-myofascial release, using either a roller or other tools of the trade, if you use enough force, not too much, you can feel the tissue twitch, contract, and then release when it’s stimulated properly. This release is why it’s called Myofascial Release instead of “Rip the Shit Apart” or “Stretch the Shit Apart.”
In my opinion, the main effect of foam rolling or any other SMR technique is in modulating the neural tone of the area, which produces the range of motion changes compared to stretching. This change in tone allows the muscle to move differently than before, usually with greater range of motion and a similar force production capability compared to before rolling. Some studies have shown prolonged stretching to produce similar range of motions can reduce force production short term following the stretch, which if you’re using it as a means of increasing range of motion before a workout could be counter productive. If you were to use long hold stretching following a session, more power to you.
If you’re interested in learning more about foam rolling, the science and actual application of it, my video series Foam Rolling 101 is an awesome resource to cover these bases. It discusses more indepth anatomy, physiology, and has a breakout session to show how to hit the major sections of the body for the best release work possible. It’s even cheap too, with 6 hours of HD video for only $67.
2 Responses to Foam Rolling Isn’t Stretching, But It’s Still Important