A Primer on Pain
Today’s post is a guest post from Matthew Danziger. The main reason why I wanted Matt to write a post is based on a pretty cool story.
Matt purchased Post Rehab Essentials V.2.0 as soon as it was released. In it, I had a small section discussing the importance of having at least a rudimentary understanding of pain and why it’s a big deal when working with people who have injuries or issues with movements.
Well, Matt is way smarter than I am when it comes to that kind of thing, and he rightly challenged some of the clumsy and less than elegant ways I approached the concept, as well as some of the concepts that I may have gone through too quickly and not given enough salient information to help trainers make better decisions.
We had some really good discussions through email where he gave me some excellent pointers, resources and info on some of the current thought processes regarding pain.
He’s way ahead of the curve for a lot of trainers out there in regards to how he looks at pain, and I wanted to have him share his thoughts to get a broader audience. I’m sure you’ll get a lot out of it, whether you have injuries, chronic pain, or merely know someone who is dealing with the same. Enjoy, and play nicely with Matt.
Pain is a subject that’s very personal to me. For about half of my 26 years I’ve suffered from varying degrees of chronic pain that has substantially altered the course of my life. In dealing with this I’ve seen PTs, OTs, DCs, MDs, and LMTs. I’ve tried ART, IASTM, PRI, IMS, SMR, and LMNOP. That last one might not be real. Each of these things helped in varying degrees and I am grateful to everyone who took the time to try to help me in a time of need. However, one thing that was distinctly lacking throughout this process was education on pain. Understanding pain has greatly empowered me in managing it, which is why I’m so passionate about pain education for others. I hope that by the end of this article that readers will have a greater understanding of what pain is so that they too can break free from its hold.
Clinical and research physiotherapist Dr. Lorimer Moseley defines pain as “… a multiple system output activated by an individual specific pain neurosignature; the neurosignature is activated whenever the brain concludes that the body tissues are in danger and action is required.” That’s a mouthful, but there’s a lot of really interesting and important stuff there so let’s break it down.
Pain is an output of the brain
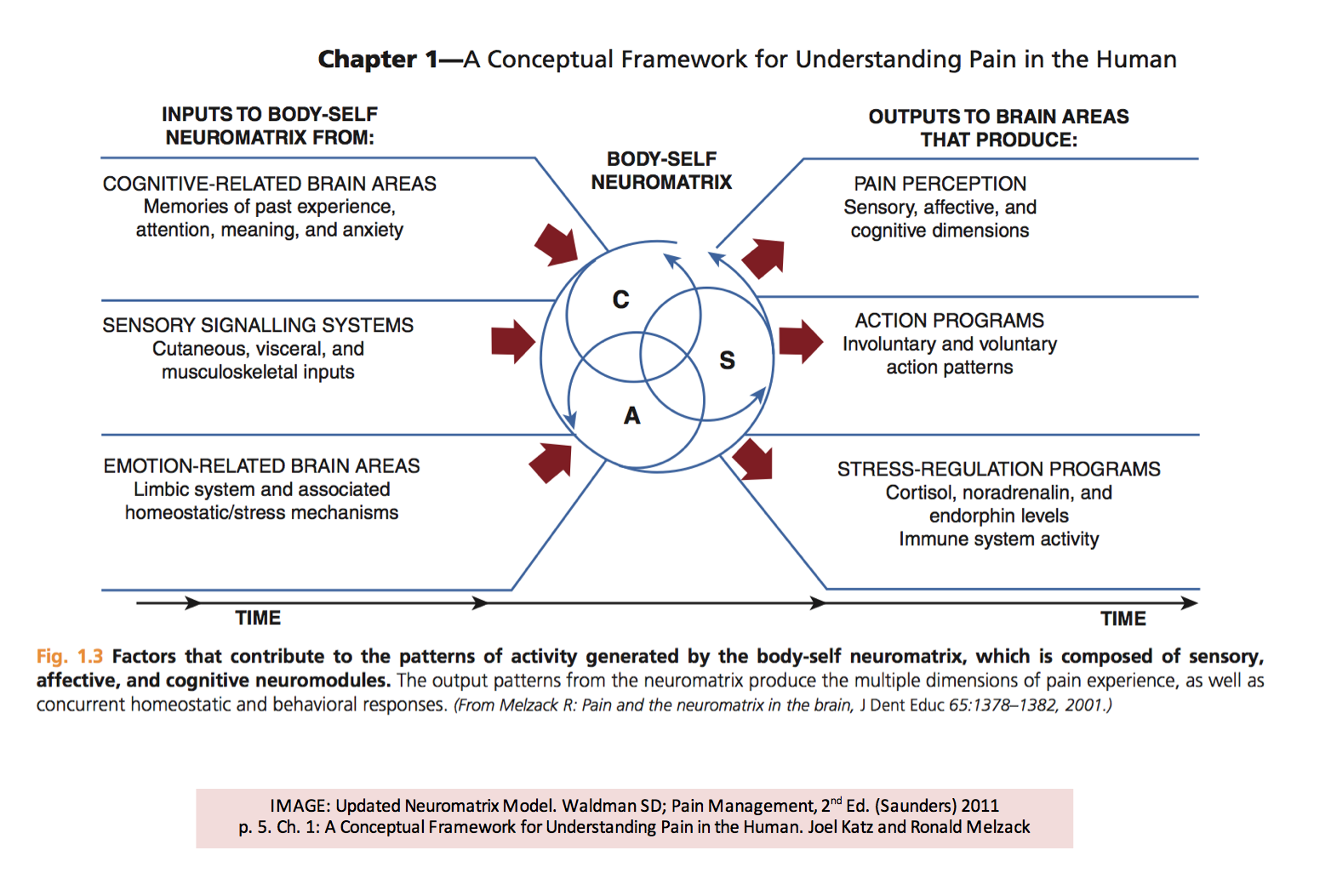
There is no such thing as a pain receptor or pain fiber. Pain is the result of a large variety of inputs to the system and it does not exist unless the brain has decided it is necessary to create pain to motivate a change in behavior or action. This idea is best illustrated by the pioneering pain researcher Ronald Melzack’s Neuromatrix theory of pain.
To put this another way, pain is the result of the brain’s opinion of a perceived threat to the body. Pay special attention to the words perceived and opinion because pain, much like our senses, can be a poor indicator of reality. An example of how easily the brain can be fooled is seen below.
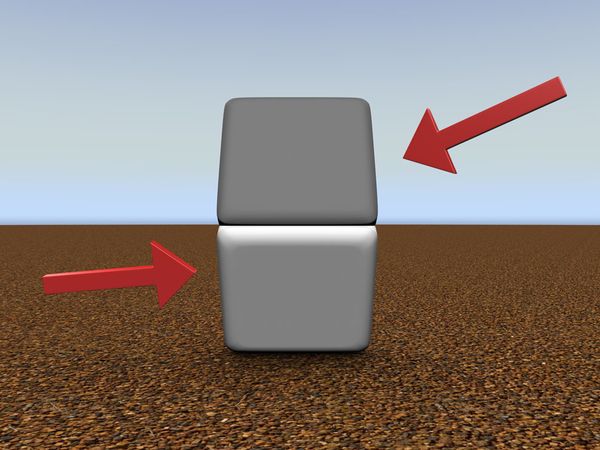
For most people the top block will appear to be darker than the bottom block. Cover the dividing line with your finger and you will see that the blocks are the same color.
In this optical illusion you can clearly see how you can be tricked into seeing something that isn’t accurate. This is because sight is the output of a complex process, which is informed by how you interpret the light hitting your eyes based on context, culture, beliefs, expectations, previous experiences, etc. Pain functions much the same way. However, with vision it’s well understood that the light that enters your eye is the catalyst for sight. Pain is not as straightforward.
Pain is very complicated
Claiming to know with certainty why different people do or don’t experience pain even in nearly identical situations is either unfounded or dishonest. The next time anyone tells you that anything “causes pain” you should give them a skeptical glance.
To be perfectly clear, tight/short/weak muscles, bad posture, dysfunctional movements, unstable joints, asymmetries, bad alignments, anything to do with fascia, or muscle imbalances do not directly cause pain. Some of these things may result from pain, [or] lead to injury or decreased performance, but many of them have been shown to have little or no relevance to pain, and other ideas are informed speculation at best. This is not to say things don’t change for the better when approaches that focus on these things are used, but if they work it’s probably not for the reasons typically given. To learn more about research on these ideas, check out the writing of Paul Ingraham (http://saveyourself.ca/) and Greg Lehman (http://www.thebodymechanic.ca). I know what I just said goes against a lot of beliefs out there, but it is consistent with what research demonstrates. Pain is far too complex to identify a single cause.
One of the only contributing factors I am confident identifying in the creation of pain is nociception. Nociceptors are sense receptors present throughout the entire body in nervous tissue that act like tiny threat detectors. Nociception is created when nociceptors are activated by heat, pressure, or chemicals. In most cases of chronic pain it becomes easier for the nociceptors to become activated and/or the nociceptive signals become amplified. This is known as sensitization.
So nociception causes pain and you can stop reading now, right? Sorry reader, it’s not quite that simple. To quote Moseley again,
“Nociception is neither sufficient nor necessary for pain.”
The warning signals from nociception are very frequently involved in pain, but this is like saying light entering the eyes causes vision directly. Remember how easily our eyes can be fooled. For nociception to become pain it must be perceived to be a relevant threat by the brain. This is why pain and nociception must be viewed as different phenomena.
Pain Without Nociception
In difficult cases of chronic pain sometimes surgical procedures are done to completely cut nerves around the painful site. However, in many of these cases patients still experience comparable pain at the same site. Similarly, in most cases of a lost limb, people will experience pain where their former limb once was, which is known as phantom limb pain. In these cases it is impossible for nociception to be present because there are no nerves to signal, however pain is still present.
Nociception Without Pain
Particularly in high stress situations it is not biologically advantageous to a person’s safety to experience nociception as pain. This is why soldiers who sustain very serious injuries on the battlefield often will not experience any pain until they are safely in a hospital. Recently in the NCAA, Louisville men’s basketball player Kevin Ware suffered a dramatic compound fracture to his right leg. When asked about his injury Ware said, “I didn’t feel any pain. It didn’t hurt. Honestly, it didn’t hurt.” I won’t even pretend to speak for Ware, but I would guess he felt the outcome of the game was more important than his own safety.
All of this brings me to my next point,
Pain is a poor indicator of tissue damage.
For most people paper cuts hurt a lot. Yet most people have also looked down at their hand at some point or another only to notice their hand or finger is bleeding without having felt a thing. In both cases there are similar amounts of damage to similar locations with completely different experiences. How many times have you woken up to find a bruise that you have no idea where it came from? Have you ever gotten a bad cramp? Do you know people with an “old injury” that “flares up” for a day or two even years after the healing process has finished? If experiencing pain was directly related to the amount of tissue damage present none of these things would be possible.
Additionally, a number of imaging studies have shown large percentages of completely pain free and fully functional individuals who have apparent damage, “abnormalities”, or degeneration. Backs were found with bulging discs, stenosis, herniations, and nodes. Shoulders were found with partial or full thickness tears of the rotator cuff. Hips were found with with torn labrums. Knees were found with meniscal degeneration or tears. Arthritis has been found in a variety of places. Yet all of the people imaged had no pain at all, and many were even athletes performing at high levels. No one knows for sure what determines the amount of pain created, but researchers over the past 30 years have hit on something big.
Beliefs about pain impact pain
While it’s always worth seeing a professional to rule out pathology, once you accept that pain is not necessarily related to anything biomechanically “wrong” or physically damaged, then you can begin to accept that maybe your pain is a result of a cranky nervous system. Or that a cranky nervous system is amplifying the nociception that may be coming from the tissues. Thus you can have damage but you don’t always have to have pain. Remember that pain is an opinion based on perceived threat, so your beliefs, fears, expectations, and outlook can heavily impact how threatening a stimulus may be. This is probably why people with depression have a much higher incidence of pain. There are even some cases where beliefs alone have been shown to cause a great deal of pain.

In this case study, a builder was admitted to the ER because a large nail was driven through the bottom of his boot. He was in such debilitating pain that he needed to be sedated for the nail to be removed. After the removal of his boot it was discovered that the nail had gone between his toes and had not left a scratch.
Note from Dean: It’s a situation that’s similar to but somewhat different from this movie clip:
Consider being told that you have a bulging disc in your low back. If you thought this was a terrible thing that meant your spine would break if you bent over then there’s a good chance that your level of perceived threat would be greatly elevated. This belief could function very similarly to the nail through the boot. This is why I want to scream when people attribute pain to simple linear causes.
Now imagine being told that the bulging disc in your low back is one of many findings present in a large percentage of the population that is completely asymptomatic and pain free. Consider that there is good reason to suspect that a bulging disc might be as relevant to pain as gray hair, wrinkles, or anything else in the regular aging process. Besides being accurate, this is a belief that facilitates confidence, self-efficacy, and recovery. There’s some really good news in all of this.
Understanding pain is useful in both the treatment and prevention of pain
There is an ever growing body of research that shows that pain education alone or in conjunction with other rehabilitative treatments produce favorable results even where many others have failed. There is even some promising evidence that understanding pain can be useful in the prevention of pain. All of this is especially important in cases of chronic pain where many people could previously find no relief and offers great hope for the future of treatment and prevention. Even that hope alone might do wonders for those who are suffering.
In Conclusion
Pain is an output of the brain based on its opinion of a perceived threat to the body. However, pain is poorly correlated with actual tissue damage. Most pain becomes present when a physical and/or mental stimulus is decided to be particularly threatening to the body based on experiences, culture, beliefs, expectations, and context. If you are able to resolve nociception and/or change the way you understand pain, then even difficult chronic pain can be successfully treated.
FAQ
So is pain is all in your head?
The phrase “all in your head” is accurate in the same way that everything else performed by the brain is all in your head, but it has come to mean imaginary or not real. Pain is ALWAYS real no matter what the cause, and anyone who says otherwise should be ignored and mocked vigorously.
Should I ignore pain?
Pain is unpleasant, but it is also very important for survival. People who are born without the capacity to feel pain die very young because they are completely unable to identify potentially threatening situations. Ignoring pain will not make it go away and it will often make things worse. It’s always worth seeking care from someone who understands the treatment of pain.
Are you saying biomechanics and injuries don’t matter?
There is no clear causal relationship between either of these things and pain, but both can affect an individual’s physical capabilities and quality of life. Pain and injuries are both important, but the terms cannot be used interchangeably.
References:
Pain and the Neuromatrix in the Brain. (http://www.ncbi.nlm.nih.gov/pubmed/11780656)
A pain neuromatrix approach to patients with chronic pain. (http://www.ncbi.nlm.nih.gov/pubmed/12909433?dopt=Abstract&holding=f1000,f1000m,isrctn)
Cellular and Molecular Mechanisms of Pain (http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2852643/)
The fall of the postural-structural-biomechanical model in manual and physical therapies: exemplified by lower back pain. (http://www.ncbi.nlm.nih.gov/pubmed/21419349)
Magnetic resonance imaging of the lumbar spine in people without back pain. (http://www.ncbi.nlm.nih.gov/pubmed/8208267)
Magnetic Resonance Imaging of the Asymptomatic Shoulder of Overhead Athletes
A 5-Year Follow-up Study (http://ajs.sagepub.com/content/31/5/724.short)
Efficacy of classification-based cognitive functional therapy in patients with non-specific chronic low back pain: A randomized controlled trial. (http://www.ncbi.nlm.nih.gov/pubmed/23208945)
Brief psychosocial education, not core stabilization, reduced incidence of low back pain: results from the Prevention of Low Back Pain in the Military (POLM) cluster randomized trial (http://www.biomedcentral.com/1741-7015/9/128)
Further Information
Introductory
Anything with Lorimer Moseley and/or David Butler. There are many great YouTube videos available where they discuss pain using funny stories and easy to follow examples. They also have a fantastic book called “Explain Pain”
The ongoing series “Empowering Self Management of Pain” by PainBC http://www.youtube.com/user/PainBC
In Depth
There is no better resource on the web for understanding pain than the forums at www.SomaSimple.com There you are safe, but your ideas are not. Be prepared to defend what you say if you post, but if you stick around you will learn more in less time than many do in years of university study.
Research and writing by:
Ronald Melzack, Patrick Wall, Peter O’Sullivan, Eyal Lederman, Max Zusman, Vilayanur S. Ramachandran, Barrett Dorko, Diane Jacobs
Acknowledgments: I want to thank everyone who helped fact check and edit this article and a special thank you to Dean Somerset for running it.

Matthew Danzinger is a personal trainer in Manhattan, Queens and Long Island who owns and operates True Movement, a company dedicated to helping people move and feel better. His true passion is helping people recover from injuries, and is able to hang with the best in the business when discussing pain and pain management. Great post, Matt.
17 Responses to A Primer on Pain